Yu-Yan Jiao1,
Yu-Zhen Shen1,
Yan Liu4,
Hua Yan2,
Jing Wang3,
Jian-Zhe Li1 ![]()
For correspondence:- Jian-Zhe Li Email: ljzlijz@163.com
Received: 22 June 2016 Accepted: 6 November 2016 Published: 22 December 2016
Citation: Jiao Y, Shen Y, Liu Y, Yan H, Wang J, Li J. Clinical efficacy of radiotherapy combined with sodium glycididazole in the treatment of recurrent oesophageal carcinoma. Trop J Pharm Res 2016; 15(12):2719-2723 doi: 10.4314/tjpr.v15i12.26
© 2016 The authors.
This is an Open Access article that uses a funding model which does not charge readers or their institutions for access and distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0) and the Budapest Open Access Initiative (http://www.budapestopenaccessinitiative.org/read), which permit unrestricted use, distribution, and reproduction in any medium, provided the original work is properly credited..
Purpose: To assess the clinical efficacy and side effects of radiotherapy combined with sodium glycididazole in the treatment of recurrent esophageal carcinoma.
Methods: Ninety patients with locally recurrent oesophageal carcinoma who were admitted to the Oncology Department at Taian City Central Hospital, Shandong, China, were randomly divided into a treatment group (treated with radiotherapy and sodium glycididazole) and a control group (treated with radiotherapy alone) in a randomized study. Short-term curative effects, median progression-free survival (PFS), and side effects were compared between the two groups.
Results: The cure rate in the treatment group was 86.70 %, whereas that in the control group was 51.10 % (p < 0.05). Median PFS in the treatment group was 9.9 months versus 5.3 months in the control group (p < 0.05). Side effects in both groups included alopecia, headache, nausea, vomiting and leucopaenia, at level one or two. In this regard, the difference between the two groups was statistically insignificant (p > 0.05).
Conclusion: Radiotherapy combined with sodium glycididazole shows a higher short-term curative effect in the treatment of recurrent oesophageal carcinoma than radiotherapy alone.
Introduction
Oesophageal carcinoma is a common gastrointestinal tract cancer and has high morbidity and mortality among malignant cancers [1,2]. Today, surgery is the major treatment method for oesophageal cancer [3,4]. However, the anatomical structure of the oesophagus causes skip metastasis in lymph nodes, making the elimination of lymph nodes during surgery more difficult. Thus, operative treatment alone does not control recurrence and metastasis of the disease and typically results in unsatisfactory long-term effects. Postoperative local recurrence and distant metastasis contribute to this failure of surgical treatment [5,6].
More than 40 % of patients are likely to have mediastinal lymph node metastasis or anastomotic recurrence after undergoing radical resection for oesophageal carcinoma, but it is often difficult for recurrent patients to undergo further surgery; thus, radiotherapy becomes the main treatment method [7]. However, radiotherapeutic effects are less than ideal. One of the main factors influencing radiotherapeutic efficacy is the insensitivity of 10 – 50 % of hypoxic cells in a solid carcinoma to low linear energy transfer (LET) rays [8]. It has been shown clinically that many chemotherapy drugs can increase sensitivity; however, there are some adverse effects [9]. Sodium glycididazole, the only formally clinically used radiosensitiser with high efficacy and low toxicity, is a safe and effective radiosensitiser for hypoxic cells. In this study, we treated recurrent oesophageal cancer using radiotherapy combined with sodium glycididazole and obtained significant short-term effects.
Methods
Ninety patients with confirmed recurrent oesophageal carcinoma, who were admitted to the Oncology Department at Taian City Central Hospital, Shandong, China from May 2013 to May 2015 were enrolled. Out of the number, there were 54 men and 36 women (age range, 39 – 79 years, mean age, 56.7 ± 2.3 years). Karnofsky performance status scores of the patients were all > 70 points; the diameter of the tumour was from 1.8 – 6.1 cm and the average tumour volume was 88 cm2. The regional lymph nodes metastasis rate was 74.40 %, among which cervical lymph node metastasis accounted for 16.70 %, mediastinal lymph node metastasis for 25.60 %, cervical lymph node metastasis and mediastinal lymph node metastasis for 22.20 %, and anastomotic recurrence for 7.80 %. Patients were divided randomly into a treatment group (45 patients treated with radiotherapy and sodium glycididazole) and a control group (45 patients treated with radiotherapy alone).
This study was approved by the Medical Ethics Committee of Taian City Central Hospital (approval no. TCCH20151004JYY) and followed the guidelines of the Declaration of Helsinki [10]. All patients provided written informed consent.
Radiotherapy plan
Three-dimensional intensity modulated radiation therapy and 6-MV X-ray conventional segmentation treatment were used. Patients were given 1.8 – 2 Gy each time, five times per week. The total radiation to the gross tumour volume was 60 – 66 Gy, while that to the clinical target volume was 50 – 50.4 Gy.
Sodium glycididazole was provided by Shandong Green Pharmaceutical Co., Ltd., China. Sodium glycididazole for injection (800 mg/m2) was dissolved and diluted with 100 mL normal saline. Patients were given an intravenous infusion over 30 min. Patients then received conventional radiotherapy within 120 min. This process was repeated three times per week until the end of radiotherapy.
Patients in the treatment group were treated with radiotherapy and sodium glycididazole; those in the control group were treated with radiotherapy alone.
Evaluation of clinical and side effects
In evaluating the response to radiotherapy, we used the Response Evaluation Criteria in Solid Tumours (World Health Organization) [11]. Complete remission (CR) referred to the disappearance of all target tumours. Partial remission (PR) meant that the size of target tumours was reduced by 30 %. Stable disease (SD) meant that the reduction in the size of the target tumours did not reach the standard for partial remission and the increase did not reach the standard for progression. Progressive disease (PD) meant that the size of the target tumours increased by 20 % or there were new lesions. The formula for the overall effective rate was: overall effective rate = (number of cases of complete remission + number of cases of partial remission) / total number of cases.
Adverse reactions were divided into four levels according to the National Cancer Institute Common Terminology Criteria for Adverse Events (ver. 3.0; NCI-CTC). Progression-free survival (PFS) was defined as the period from the beginning of radiotherapy to the death of patients.
Statistical analysis
Data were analysed using SPSS software (ver. 20.0, IBM, Armonk, NY, USA) and further assessed using χ2 tests. The data are expressed as percentages (%). Comparison of data between the two groups was made using t-tests. The data are expressed as mean ± standard deviation (SD). For survival analysis, we used Kaplan–Meier method. P < 0.05 were taken to indicate statistical significance.
Results
Clinical effects
Complete remission rates in the treatment and control groups were 26.70 % and 17.80 %, respectively (χ2 = 1.157, p > 0.05). There was no significant difference between the groups. Overall response rates (CR + PR) were 88.90 % and 51.10 % respectively; there was a significant difference between groups (χ2 = 5.03, p < 0.05). Specific results are provided in .
Analysis of survival rate
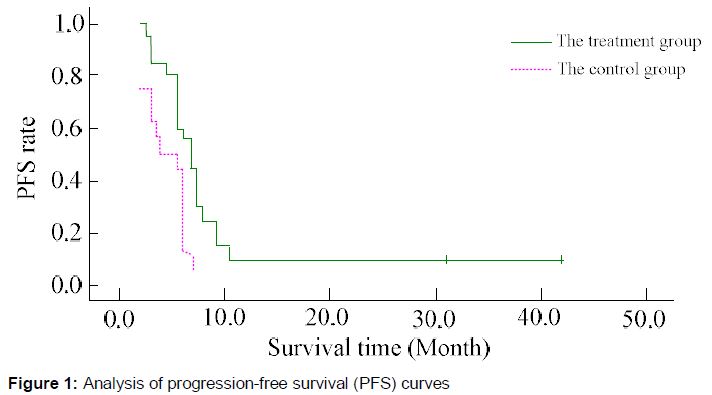
The median PFS in the treatment group was 9.9 months (95 % confidence interval (CI) = 5.13 – 14.67 months), whereas that of the control group was 5.3 months (95 % CI = 3.16 – 7.48 months); the difference was statistically significant (p < 0.05; ).
Side effects in both two groups included alopecia, headache, nausea, vomiting, and leucopaenia. The difference between the two groups was statistically insignificant (p > 0.05). Alopecia was at level two, and the other reactions were at level one (Table 2). There was no level three or four side effect. No serious organ damage occurred.
Discussion
Anastomotic recurrence and/or mediastinal lymph node metastasis are the major reasons why patients who undergo oesophageal carcinoma operations die after 2 – 3 years. By analysing 175 patients with recurrent oesophageal carcinoma who underwent three-field operations, Li et al [12] found that the lymphatic metastasis rate was 90.29 %, the anastomotic recurrence rate was 19.43 %, and the tumour area recurrence rate was 9.71 %. Among lymph node metastases, mediastinal lymph node metastasis at the superior mediastinum was the most commonly seen; abdominal lymph node metastasis is common with lower thoracic oesophageal carcinomas.
Zhu et al [13] analysed recurrence retrospectively in 98 cases of oesophageal carcinoma and found that lymph node metastasis ranked first, anastomotic recurrence second, and tumour area recurrence was the least common.
Regarding treatment modalities for patients with recurrent oesophageal carcinoma, radiotherapy is the main method, but its clinical effects are unsatisfactory, which is considered to be related to hypoxia in cancer cells. Hypoxia, a common phenomenon in solid tumours, weakens radiotherapeutic efficacy by decreasing apoptosis [14]. Sodium glycididazole is a new nitroimidazole compound that increases the sensitivity to radiation. The drug has no anti-cancer effect per se; however, it can increase the sensitivity of hypoxic cells to radiotherapy and chemotherapy. The sensitivity mechanism of sodium glycididazole involves (1) strong damage and electron fixation and (2) suppression of DNA repair enzymes to tumour cells. Specifically, ionising radiation damages the tumour cells. The electrophilic group of sodium glycididazole captures electrons from damaged tumour target molecules. This promotes the generation of radical cations, accelerating the death of tumour cells. The suppression of DNA repair enzymes in tumour cells, especially polymerase B, strengthens the killing function in tumour cells by stopping DNA replication. This, in turn, decreases the oxygen dependence during the killing of tumour cells, suppressing potentially lethal and sub-lethal damage repair.
While sodium glycididazole can increase the sensitivity of tumour cells to radiotherapy and chemotherapy, it does not affect normal cells [15]. Additionally, it is characterised by high safety and efficacy because it does not accumulate in the patient’s body. Previous clinical studies have shown that the drug can greatly increase the sensitivity of cells in head and neck neoplasms and oesophageal carcinoma, and it has good short-term effects [16-19].
A previous study compared the clinical effects of radiotherapy combined with sodium glycididazole and radiotherapy alone in the treatment of patients with brain metastases from breast carcinomas. The response rates in the treatment and control groups were 88.90 % and 51.10 %, respectively; the difference was significant. The median PFSs of the two groups were 9.9 and 5.3 months, respectively; the difference was statistically significant.
Our results showed that treating patients with recurrent oesophageal carcinoma with radiotherapy and sodium glycididazole had positive effects, which were better than those in the control group. Moreover, we found no significant difference between the two groups in terms of side effects, such as alopecia, headache, nausea, vomiting, and bone marrow suppression (p > 0.05). All patients could tolerate the side effects; none of the patients discontinued treatment, suggesting that sodium glycididazole did not aggravate any adverse reaction.
Limitations of the study
The sample size in the study was small; thus, prospective clinical studies with larger sample sizes are required. Also, although there was an obvious difference in median PFS between the two groups, the research period was only 4 years. We were unable to show whether there was also a difference in longer-term PFS. Thus, the duration of follow-up needs to be extended in future studies.
Conclusion
Sodium glycididazole in combination with radiotherapy was more effective clinically in treating patients with local oesophageal carcinoma recurrence than radiotherapy alone. Moreover, the combined therapy did not aggravate side effects.
Declarations
Acknowledgement
References
Archives


News Updates